Ob Gyn History Template
Ob Gyn History Template - If your menstrual periods are regular; Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. If so, what was the diagnosis and when? Medical history questionnaire department of obstetrics & gynecology division of reproductive endocrinology & infertility name: Any history in you or your sexual partner(s) of syphilis, sores, gonorrhea, herpes, blisters, trichomonas, warts, pelvis or tubal inflammation (pid), or other sexually transmitted diseases?. Department of obstetrics and gynecology patient history questionnaire ucla form #11864 rev. What birth control method(s) do you currently use? What day was your pregnancy test first. Obstetrical history including abortions & ectopic (tubal) pregnancies. Do you normally have a period every month? Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number can we leave a secured voice mail? The document outlines a comprehensive patient assessment. Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. Find items in uic library collections, including books, articles, databases and more. Department of obstetrics and gynecology patient history questionnaire ucla form #11864 rev. Have you ever been diagnosed with a medical or psychological condition? Have you had any bleeding since your last period? Any history in you or your sexual partner(s) of syphilis, sores, gonorrhea, herpes, blisters, trichomonas, warts, pelvis or tubal inflammation (pid), or other sexually transmitted diseases?. No need to install software, just go to dochub, and sign up instantly and for free. If you have previously filled out the updated version,. If your menstrual periods are regular; What was the first day of your last normal period? If so, what was the diagnosis and when? _____ lmp _____ edd _____ by _____ Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. Up to 40% cash back edit, sign, and share ob gyn history and physical sample online. Any history in you or your sexual partner(s) of syphilis, sores, gonorrhea, herpes, blisters, trichomonas, warts, pelvis or tubal inflammation (pid), or other sexually transmitted diseases?. Find items on the uic library website, including research guides, help articles, events and. If so, what was. (03/11) page 1 of 4 mrn: Up to 40% cash back edit, sign, and share ob gyn history and physical sample online. Any history in you or your sexual partner(s) of syphilis, sores, gonorrhea, herpes, blisters, trichomonas, warts, pelvis or tubal inflammation (pid), or other sexually transmitted diseases?. Department of obstetrics and gynecology patient history questionnaire ucla form #11864 rev.. Find items on the uic library website, including research guides, help articles, events and. What day was your pregnancy test first. What was the first day of your last normal period? Any history in you or your sexual partner(s) of syphilis, sores, gonorrhea, herpes, blisters, trichomonas, warts, pelvis or tubal inflammation (pid), or other sexually transmitted diseases?. The document outlines. Find items in uic library collections, including books, articles, databases and more. Do you normally have a period every month? Any history in you or your sexual partner(s) of syphilis, sores, gonorrhea, herpes, blisters, trichomonas, warts, pelvis or tubal inflammation (pid), or other sexually transmitted diseases?. Have you ever been diagnosed with a medical or psychological condition? (03/11) page 1. Obstetrical history including abortions & ectopic (tubal) pregnancies. If your menstrual periods are regular; Have you had any bleeding since your last period? The document outlines a comprehensive patient assessment. Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. Have you had any bleeding since your last period? If you have previously filled out the updated version,. If your menstrual periods are regular; Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. What day was your pregnancy test first. Obstetrical history including abortions & ectopic (tubal) pregnancies. If so, what was the diagnosis and when? If your menstrual periods are regular; Any history in you or your sexual partner(s) of syphilis, sores, gonorrhea, herpes, blisters, trichomonas, warts, pelvis or tubal inflammation (pid), or other sexually transmitted diseases?. Do you normally have a period every month? What was the first day of your last normal period? Do you normally have a period every month? (03/11) page 1 of 4 mrn: If you have previously filled out the updated version,. Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. _____ lmp _____ edd _____ by _____ What was the first day of your last normal period? Ob / gyn history form name date of birth age date with whom may we discuss test results or therapies?_____ at what phone number can we leave a secured voice mail? What birth control method(s) do you currently use? Have you ever been. The document outlines a comprehensive patient assessment. Obstetrical history including abortions & ectopic (tubal) pregnancies. What day was your pregnancy test first. Obstetrics and gynecology medical history questionnaire ***please note that we have updated this form in 2020. If your menstrual periods are regular; No need to install software, just go to dochub, and sign up instantly and for free. What birth control method(s) do you currently use? Have you had any bleeding since your last period? _____ lmp _____ edd _____ by _____ If you have previously filled out the updated version,. Find items in uic library collections, including books, articles, databases and more. Any history in you or your sexual partner(s) of syphilis, sores, gonorrhea, herpes, blisters, trichomonas, warts, pelvis or tubal inflammation (pid), or other sexually transmitted diseases?. If so, what was the diagnosis and when? Medical history questionnaire department of obstetrics & gynecology division of reproductive endocrinology & infertility name: This document outlines the components of an obstetrics and gynecology history taking, including sections on introduction/demographics, menstrual history, present pregnancy history, past. Find items on the uic library website, including research guides, help articles, events and.
Ob History And Physical Template Card Template

Fillable Online hhtxl Ob Gyn History And Physical Template. Ob Gyn

OBGYN Patient History Form Template OnTask
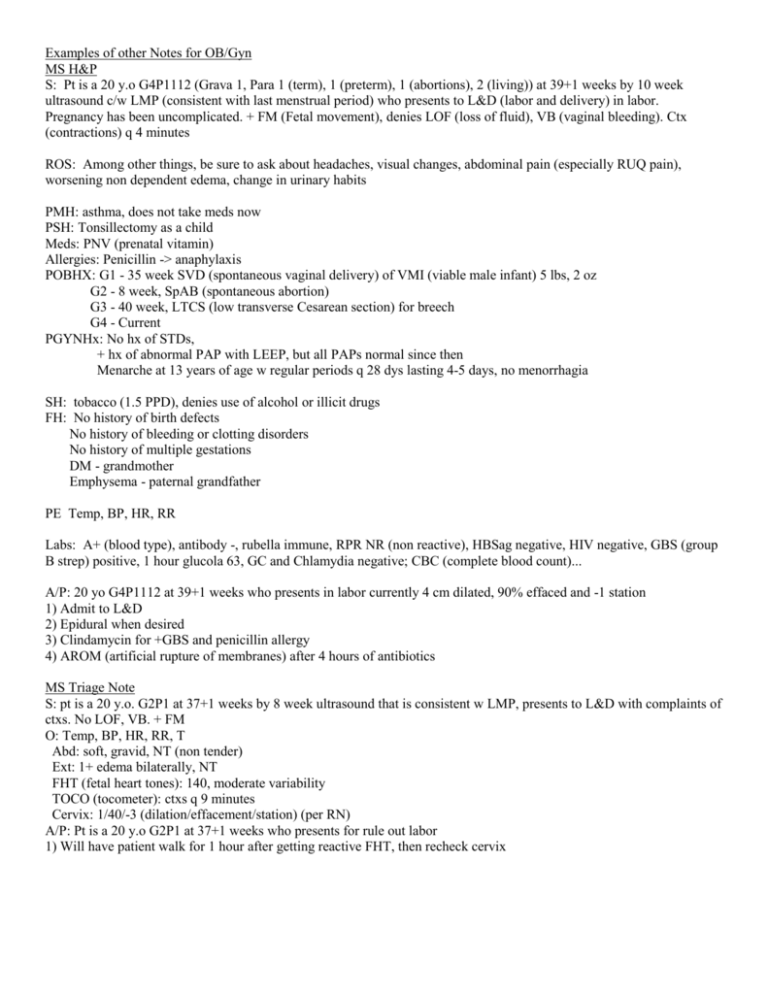
OB/GYN Medical Notes Patient History, Delivery, PostOp
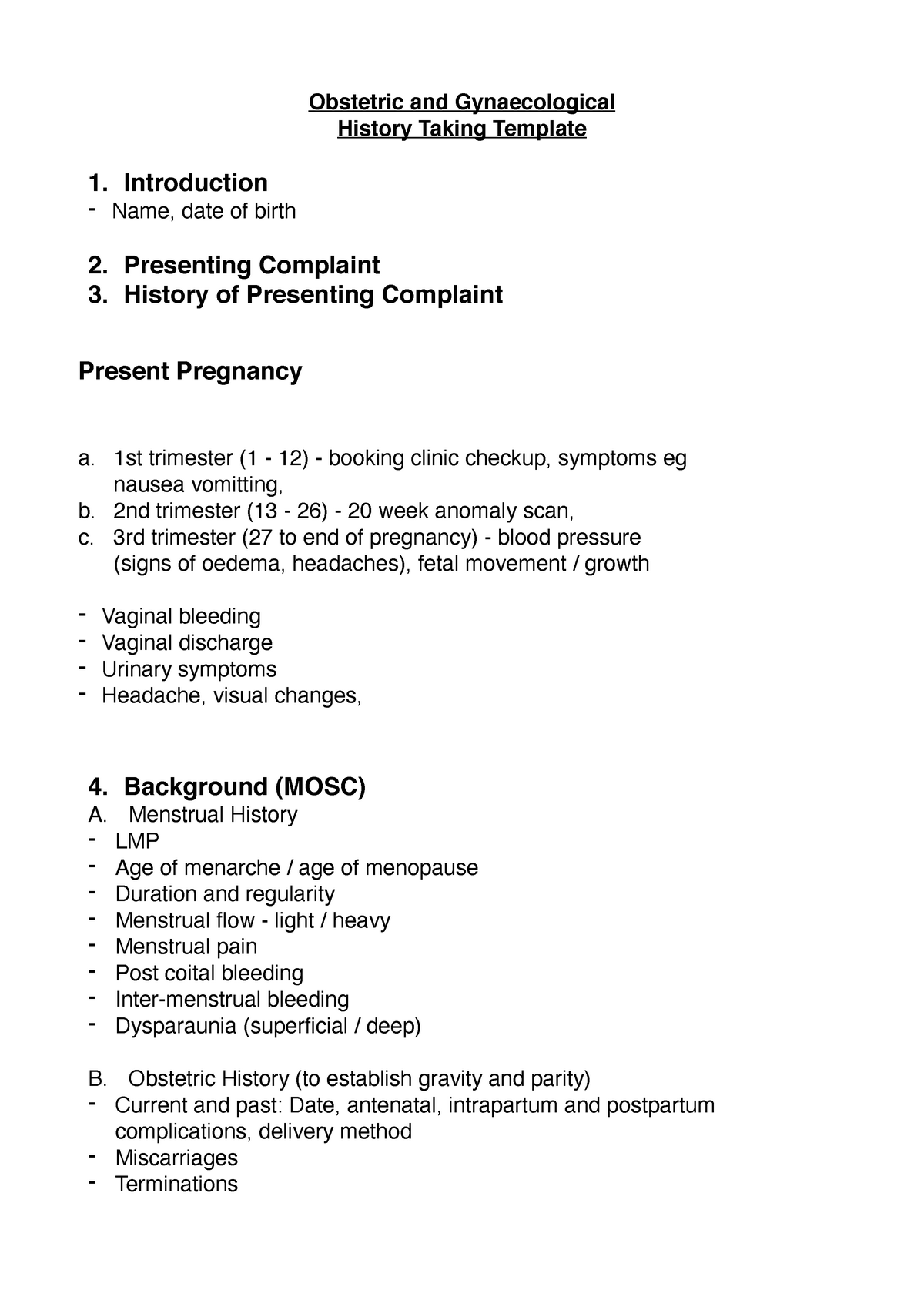
Obstetrics and Gynaecology Hx Taking Notes Obstetric and
Ob Gyn History Template
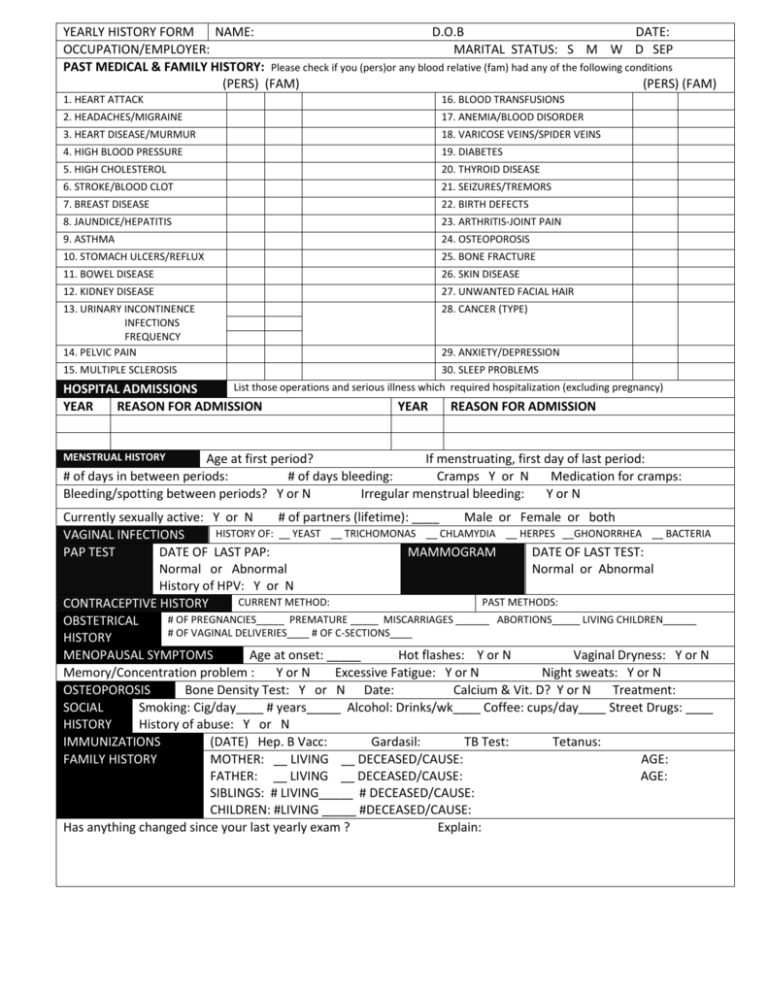
Ob/gyn History Form printable pdf download

Highland OB/GYN Patient Medical History Form 20122022 Fill and Sign
Obgyn History Template
Ob Gyn History Template
Ob / Gyn History Form Name Date Of Birth Age Date With Whom May We Discuss Test Results Or Therapies?_____ At What Phone Number Can We Leave A Secured Voice Mail?
Have You Ever Been Diagnosed With A Medical Or Psychological Condition?
Simplify Patient Intake With A Customizable Obgyn History Form.
(03/11) Page 1 Of 4 Mrn:
Related Post: